

Background: Risk stratification of venous thromboembolism (VTE) in patients with cancer is essential to evaluate the need for extended thromboprophylaxis. The Khorana score is widely used to guide VTE risk stratification in patients with cancer based on clinical parameters: cancer type, platelet count, hemoglobin level, leukocyte count, and body mass index. We sought to validate Khorana score to predict 1-year risk of VTE in a large multi-institutional, diverse, real-world cohort of patients with cancer.
Methods: Using aggregated de-identified electronic medical record data from >300 major hospitals in the in the United States (IBM Watson Explorys), we performed a retrospective cohort study of all patients who had a diagnosis of cancer. We identified cancer type, platelet count, hemoglobin level, leukocyte count, and body mass index (for calculation of Khorana score) within 7 days of cancer diagnosis and followed patients for diagnosis of VTE for 1 year post cancer diagnosis. Logistic regression models were used to evaluate association between patient characteristics and VTE risk. Receiver operating characteristics with area under the curve were used to evaluate model discrimination. All analyses were performed in Statistical Package for Social Sciences.
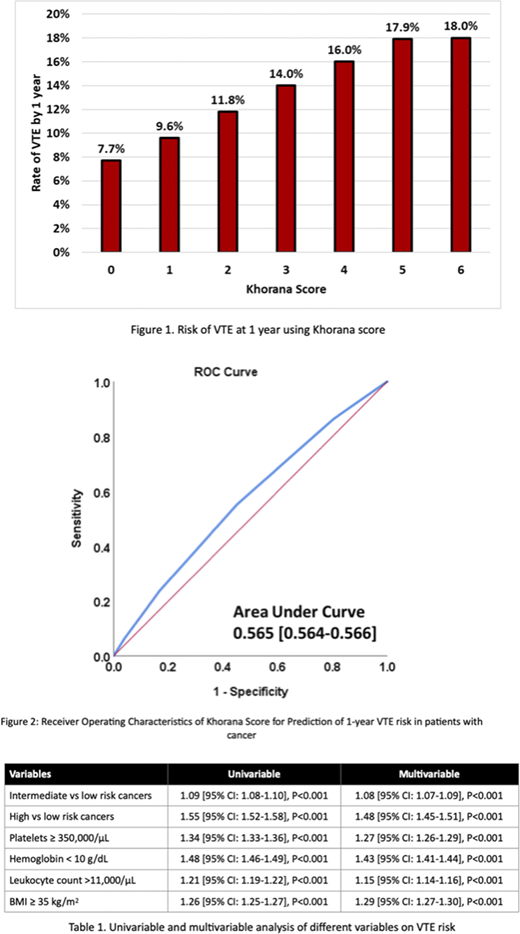
Results: A total of 2,112,260 patients with cancer were included: 52.9% females, 11.1% African Americans, 44.3% intermediate risk cancers (lymphoma, lung, breast, gynecologic, testicular and bladder), 4.5% high risk cancers (stomach and pancreas), 19.8% had Platelet counts ≥ 350,000/µL, 29% had hemoglobin <10 g/dL, 32.3% had leukocyte count >11,000/µL, and 15.1% had body mass index ≥ 35 kg/m2. Overall, 227,170 (10.8%) had a diagnosis of VTE at 1 year following cancer diagnosis. In multivariable analysis (table 1), VTE risk was associated with cancer type (intermediate vs low risk: OR 1.08 [95% CI: 1.07-1.09]; high vs low risk: OR 1.48 [95% CI: 1.45-1.51]), Platelet ≥ 350,000 (OR 1.27 [95% CI: 1.26-1.29]), hemoglobin <10 g/dL (OR 1.43 [95% CI: 1.41-1.44]), leukocyte count > 11,000 (OR 1.15 [95% CI: 1.14-1.16]), body mass index ≥ 35 kg/m2 (OR 1.29 [95% CI: 1.27-1.30]), table 1. Risk of VTE increased linearly with Khorana score between 7.7% (score = 0) to 18% (score = 6), figure 1. Khorana score had weak to modest discrimination (Area Under Receiver Operating Characteristics 0.565 [95% CI: 0.564-0.566]), figure 2.
Conclusion: In this very large real-world study of diverse patients with cancer, Khorana score was a weak predictor of 1-year risk of VTE, suggesting that VTE prediction in patients with cancer is very complex.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal